![]()
![]()
![]()
![]()
|
|
|
|
|
The Card NH3 (2-Tissue) model developed by Hutchins et al. [45] is an implementation of the irreversible 2-tissue-compartment model for cardiac PET studies using 13NH3 ammonia bolus injection. The compartment model has the following structure
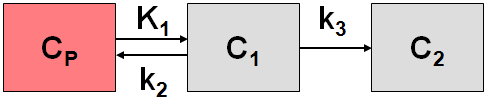
where C1 is free tracer in tissue, and C2 is metabolically trapped tracer in the form of 13N glutamine. Because ammonia is considered in this model as freely diffusible across the capillary wall, the unidirectional uptake parameter K1 equals the myocardial perfusion.
The system of differential equations is
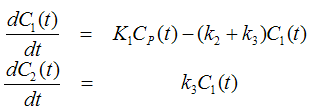
To allow the fitting of data over an extended period, the model includes the exponential metabolite correction described by van den Hoff et al. [46]
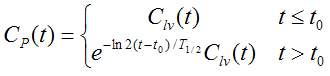
with delay t0=0.48 min and half-time T1/2=6.69 min. Clv(t) is the total tracer concentration measured in the left ventricle, including metabolites.
Additionally, the model incorporates a cardiac dual spillover correction by the operational equation

where
Vlv = spill-over fraction of the blood activity in the left ventricle Clv(t),
Vrv = spill-over fraction of the blood activity in the right ventricle Crv(t) .
Card NH3 (2-Tissue, K1/k2)
Due to the increased number of fit parameters it has been found, that the Card NH3 (2-Tissue) may suffer from identifiability problems. Therefore, the variant Card NH3 (2-Tissue, K1/k2) has been developed using the parameter K1/k2 (DV, distribution volume of free tracer is used as a fit parameter instead of k2, and k2 is derived from the estimated K1 and K1/k2. In this configuration physiological restrictions can be imposed on K1/k2 , or K1/k2 can be used as a common parameter in a coupled fit.
Implementation Notes:
Abstract [45]
"Evaluation of regional myocardial blood flow by conventional scintigraphic techniques is limited to the qualitative assessment of regional tracer distribution. Dynamic imaging with positron emission tomography allows the quantitative delineation of myocardial tracer kinetics and, hence, the measurement of physiologic processes such as myocardial blood flow. To test this hypothesis, positron emission tomographic imaging in combination with N-13 ammonia was performed at rest and after pharmacologically induced vasodilation in seven healthy volunteers. Myocardial and blood time-activity curves derived from regions of interest over the heart and ventricular chamber were fitted using a three compartment model for N-13 ammonia, yielding rate constants for tracer uptake and retention. Myocardial blood flow (K1) averaged 88 +/- 17 ml/min per 100 g at rest and increased to 417 +/- 112 ml/min per 100 g after dipyridamole infusion (0.56 mg/kg) and handgrip exercise. The coronary reserve averaged 4.8 +/- 1.3 and was not significantly different in the septal, anterior and lateral walls of the left ventricle. Blood flow values showed only a minor dependence on the correction for blood metabolites of N-13 ammonia. These data demonstrate that quantification of regional myocardial blood flow is feasible by dynamic positron emission tomographic imaging. The observed coronary flow reserve after dipyridamole is in close agreement with the results obtained by invasive techniques, indicating accurate flow estimates over a wide range. Thus, positron emission tomography may provide accurate and noninvasive definition of the functional significance of coronary artery disease and may allow the improved selection of patients for revascularization."